Collecting health data in the field is hard. Aggregating it at district, regional and national level is harder. Getting it to WHO in a format that enables global analysis across diseases, departments and countries is the kind of problem that, until recently, nobody had really solved.
The WHO Integrated Data Platform (WIDP) is the answer that emerged from ten years of iteration, collaboration and deliberate architecture. It is a DHIS2-based platform used by nine WHO departments to collect, validate, analyse and visualise health data from more than 150 countries. EyeSeeTea has been part of it almost from the beginning.
“The WIDP platform is a multi-departmental initiative where users combine their efforts, initiatives, and funds to build tools and processes that support their everyday work, ranging from data collection and approval workflows to data cleaning, validation, and reporting.”
Ryan Williams, Health Information Specialist, WHO Global Malaria Programme
What WIDP does
WIDP serves as a global data integration layer for WHO. Its core function is to give departments a shared infrastructure for collecting country data, running quality checks, and extracting information that is only meaningful at global scale. Concretely, that means:
- Data collection forms and reporting tools that allow countries to submit data directly from their national health information systems
- Spreadsheet import tools for countries that submit via Excel
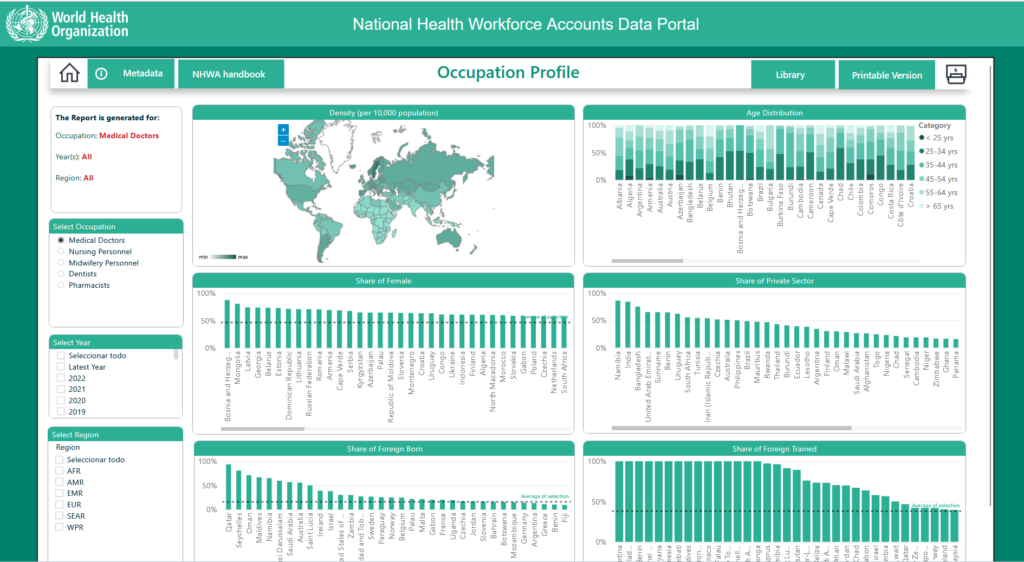
- Dashboards for visualising disease trends across countries and years
- Data export tools for statistical software analysis
- Data quality controls to validate submissions before they feed into global trend analysis
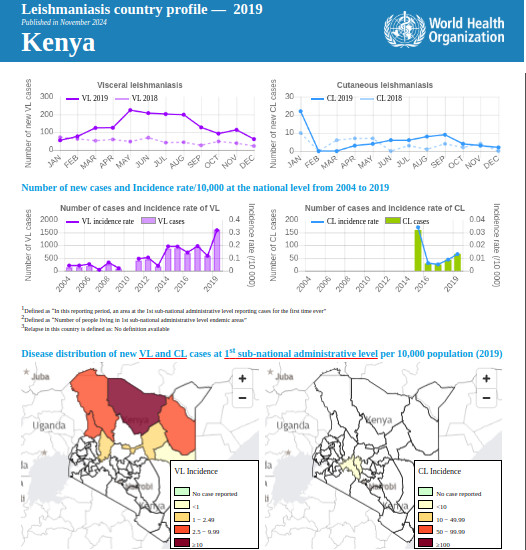
Outputs from WIDP feed into some of WHO’s most important public-facing resources: the Malaria Annual Report, the WHO Global Health Observatory, the NHWA data portal and the WHO Malaria Threat Map all draw from data collected through this platform.
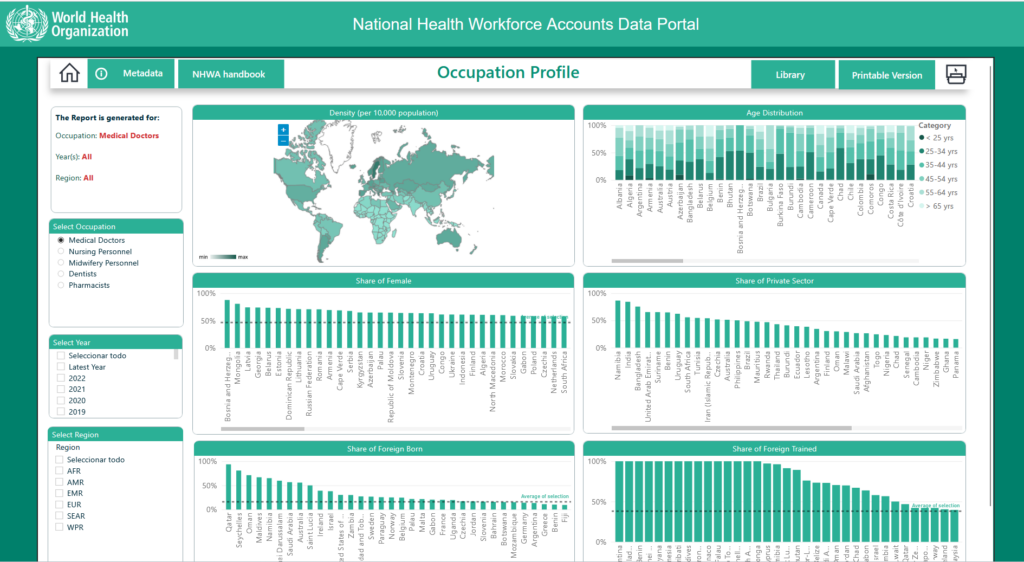
The nine WHO departments currently using WIDP are the Global Malaria Programme, Control of Neglected Tropical Diseases, Clinical Services and Systems, Health Workforce, the WHO Barcelona Office for Health Financing, Meningitis, Antimicrobial Resistance, Maternal, Newborn, Child and Adolescent Health and Ageing, and Public Health and Social Measures.
How it started: six diseases and one epidemiologist’s vision
Everything began in 2014. Lise Grout, an epidemiologist and data manager at WHO’s department for the Control of Neglected Tropical Diseases, was looking for a health information system to collect data across six different NTDs. Her colleagues were receiving data by email and phone, then entering numbers manually into Excel. She knew there were better options.
Among the systems she evaluated, DHIS2 stood out. As Grout recalls: “it was an open source system, which was also a very good point, and it was easy to develop your own metadata to use it. It was important that it was simple to use and also simple for an epidemiologist to develop the metadata and data forms. Also, Ryan Williams from the Malaria department had already started using DHIS2. It looked really promising. And the countries were already investing in DHIS2, creating the metadata, trainings… so we could leverage this to put NTDs on the health information system. This was really an opportunity for us.”
Her vision from the start went further than a single department’s needs. If DHIS2 worked for NTDs, it could work for other departments too. The same platform, the same standards, the same infrastructure, used across WHO in a way that had never been attempted before.
WIDP is now the largest DHIS2-based data collection platform within WHO, covering more than 150 countries

EyeSeeTea’s director Nacho Foche remembers that moment: “the WIDP architecture design by UPC was incredible. We saw the huge potential for the platform but also that in order to implement that design resources were needed. We were very lucky to be there almost from the start, at the right moment to establish the mechanisms and flows so that WIDP could be scalable and reliable: scripts to automate the processes, cloning schemes, reinforce security… We had been already working for some years with DHIS2 and could offer an expert vision to introduce the procedures and standardisations to comply with UPC’s designed architecture.”
Nine years on, the platform Lise Grout envisioned has become WHO’s preferred data collection tool.
Built to scale
The numbers reflect it. WIDP currently holds more than 10 million data values and one million events, across 300,000 organisational units and 300 dashboards. Thousands of new events and data values are uploaded every week, and the volume keeps growing.
Two integrations have been critical to making that scale manageable.
WIDP and other DHIS2 platforms: our Metadata Sync App facilitates the sharing of data and metadata between different DHIS2 instances, making the time-consuming processes of keeping platforms aligned significantly faster. EyeSeeTea’s Long-Term Agreement with WHO includes maintenance of Metadata Sync, ensuring it remains compatible with every new version of WIDP.
WIDP and xMART: xMART is a WHO database tool. We developed an integration that pushes country-validated data from WIDP directly into xMART, allowing data to flow across multiple WHO projects and enabling countries to share data from their national DHIS2 platforms directly into WHO’s wider data infrastructure.
Impact, in the words of the people who built it
Lise Grout explains what she set out to achieve: “there are a lot of challenges when you are collecting health data — every step is difficult, starting at the field where you have a lot of quality data issues; then to send the data from the field, to centralize the data and to send the data to WHO. The vision was to accompany the countries so we could improve quality of the data at every level: district, regional, national, so that they can improve the data quality and ease the flow because we will be using the same software, the same metadata, from and even at real time if we would want to. In this way it is not a burden anymore to get this data flowing and being able to make decisions.”
Pedro Albajar, responsible for WHO’s Chagas disease programme, puts WIDP at the centre of the fight against one of the most neglected diseases in the world:
“WIDP is the result of a pioneering open source big data project, progressively developed with the invaluable collaboration of the Polytechnic University of Catalonia, EyeSeeTea and several other institutions and organizations. Its design helped to organize and systematize the variables and sources of information for monitoring one of the most neglected tropical diseases.”

Ryan Williams, a DHIS2 pioneer from the Global Malaria Programme and one of the earliest adopters within WHO, describes what the platform has meant in practice:
“Since joining this platform, I have benefited from community support, joint development initiatives, shared experiences, and shared best practices. What is truly distinctive about WIDP is the nature of the community support, from the open-source development and the expert software knowledge and support provided by EyeSeeTea, to the collective desire to develop tools and processes that bolster our community-based approach. The platform and its tools not only serve our global objectives but are also readily adaptable for regional and country-specific use cases. My experience with the platform has been incredibly positive, as it fosters collaboration and innovation, making our work more efficient and impactful.”
A 2021 audit commissioned by WHO’s infrastructure department recommended DHIS2 as the organisation’s preferred data collection tool, a direct consequence of WIDP’s track record. As Nacho Foche puts it: “it has been so exciting to see DHIS2 use growing at WHO. WIDP’s success made other departments turn to DHIS2, so now it is the preferred data collection tool at WHO.”
Lise Grout adds one final dimension that the numbers alone cannot capture: “another very positive aspect of WIDP has been to bring together different departments who are very different and not used to working together, and see how you can maintain and manage a platform together. It was incredible to have the freedom to try different new ways of collaboration. For instance we started to have weekly meetings where we could show what was working and not working, with nearly a horizontal way to make decisions. It was such a very nice experience to work transversally.”

